
They’re both bad.
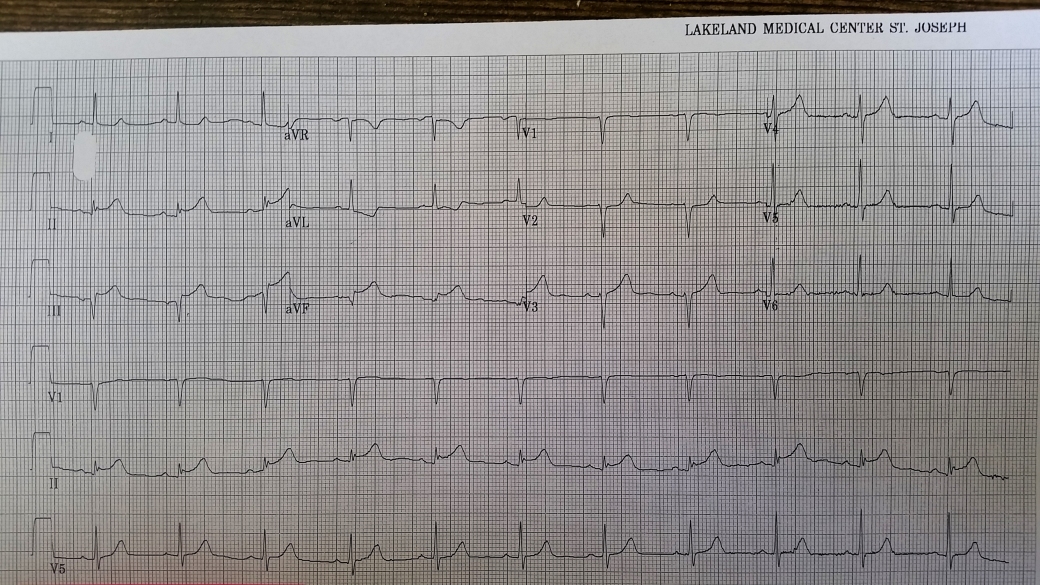
As always, we start with a systematic approach. Rate: probably around 75 based on a little over 4 big boxes. Rhythm: it’s regular, narrow complex, there’s a P before every QRS, and a QRS after every P; we see no indication of extra P waves so can likely conclude this is NSR. The PR interval looks normal, the QRS again is narrow complex. Which brings us to the ST waves
Let’s look more carefully at the inferior leads:
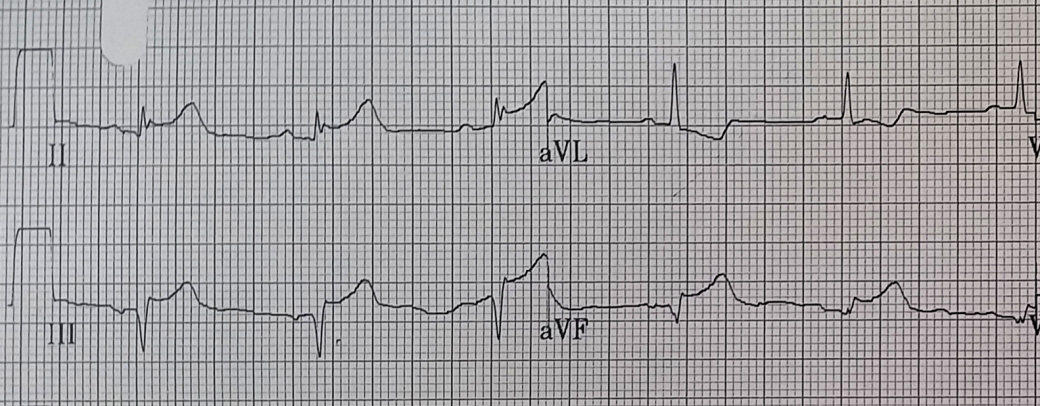
With the EKG blown up we can easily see 1-2mm of STE in II, at least 2mm in III, and about 1mm in aVF. There is also reciprocal STD in aVL.
The problem obviously is the patient’s known ascending aneurysm. About half of the responders to the quiz felt that it had likely dissected back to the RCA, the other half simply read Inferior STEMI. I don’t know that there’s any 100% way to say prospectively which it would be. I think a person would expect much larger tombstones and much more reciprocal change if the entire RCA was out but you couldn’t hang your hat on that. This would have been a difficult decision if I was at a center where I only had lytics and even though the description of the discomfort was very good for classic ischemia I probably would have gotten the CTA. Fortunately given we had a cath lab, the patient was able to go down and had their 99+% PDA lesion stented without the additional dye-load and delay; the aneurysm turned out to be a red herring.
A couple general take-homes about inferior STEMI’s: they can often be much more subtle than their anterior cousins and have far less STE. Note also that this patient is having a full-blown heart attack with upcoving ST waves. The presence of tombstones generally indicates a STEMI but STEMI can certainly happen without them. Moreover, upcoving ST waves can progress to tombstones; if there’s any doubt then repeat that EKG after 15 minutes or so!
