
Are there times when it’s hard to see? Maybe changing your shift schedule and having trouble rubbing the sleepies out of your eyes? Or staring into the sun too long trying to take dramatic pictures of your telescope?

Everything looks so yellow! How does that relate to the EKG? Read on…
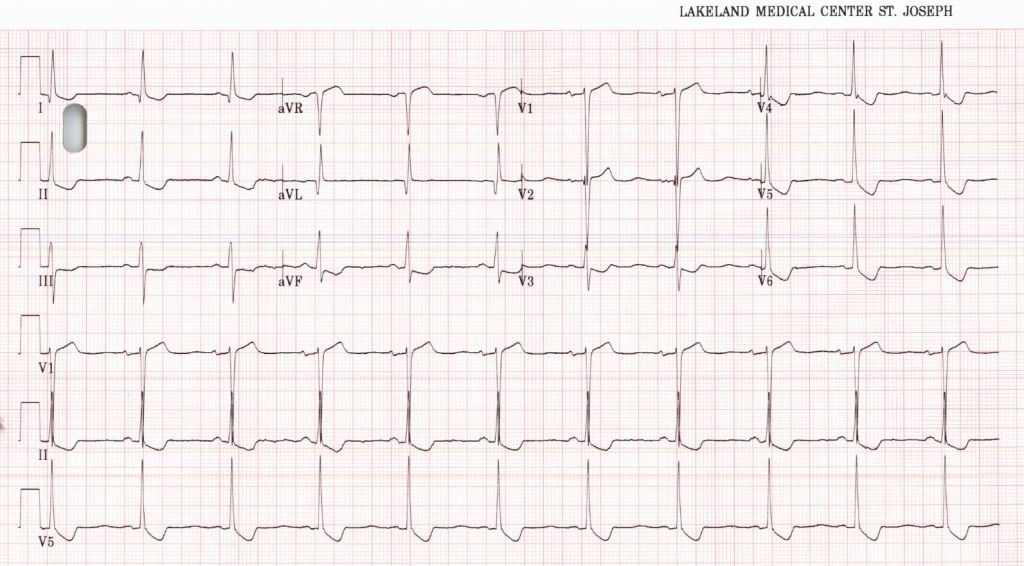
Rate looks to be in the 60’s. Rhythm is pretty obviously sinus. Axis is normal. The PR intervals are unremarkable as is the width of the QRS. There are some q waves to the lateral limb leads of unclear significance. The QRS’s do get very close to LVH criteria being 10 mm in aVL (it needs to be 11 there), and just under 7 big boxes of voltage in V2 S wave + V5 R wave (needs to be 7 big boxes). The q waves and near LVH could imply that this person does have some underlying heart disease.
The ST waves are of interest. A few of you questioned posterior MI given the shapes of the ST’s in V3 and V4. However posterior MI changes are usually most pronounced in V1 and especially V2. That scooped out shape is also present in multiple lead areas, clearly inferior and lateral, but also in V3 as well. It’s therefore a more global effect than a regional ischemia pattern. I didn’t know if the visual changes would give this EKG answer away (which per the books for many patients will be a yellowish cast to vision though I don’t know that I’ve ever asked a patient that question). There is a cardiac medication that if a person gets dehydrated and into mild renal failure can have its level rise. This person isn’t currently in Afib, but presumably they are at times; their dig level is in the mid 4’s, and the nausea and vomiting has led to an elevated Cr with a resulting elevated digoxin level.
Take-homes from this EKG with digoxin toxicity? When changes are present throughout an EKG think about global metabolic possibilities. We’re a lot more likely to think about digoxin if the patient is in Afib, but some patients’ Afib is paroxysmal and won’t always be present. Next is that scooped out shape which drew some eyes as possibly reflecting posterior STEMI. Remember that there’s always multiple things on a differential so file dig toxicity as something to think about when you think about posterior STEMI.

One thought on “So turn on the vision!”